
by Maryanne W. Waweru | May 13, 2015 | 2015, Babies, Breastfeeding, Child Care, Childhood Illnesses, Health, Kenya, World Motherhood
 Exclusive breastfeeding. Before I became a mother, I had never heard of it. I knew about breastfeeding, obviously, but not until I was seven months pregnant with my first child, did I learn it was possible to feed a baby only breastmilk for six months.
Exclusive breastfeeding. Before I became a mother, I had never heard of it. I knew about breastfeeding, obviously, but not until I was seven months pregnant with my first child, did I learn it was possible to feed a baby only breastmilk for six months.
Most mothers I knew began complementary feeding with porridge and fruits around three months–which often coincided with their return to work after their 90-day maternity leave. Many mothers in rural areas offered their babies cow’s milk or porridge by two months. Certainly, almost all babies I knew were, by four months, happily indulging in fruits and porridge — regardless of whether they were breastfeeding, taking cow’s milk, or for the privileged few, drinking formula.
Could a child survive without even a drop of water? Impossible, I thought. Insane, actually. And even if it were possible, I imagined that the child would suffer from a nutritional deficiency of some sort. But, there was a mother and child on a television news program who appeared to prove me wrong.
I was confused as I listened to that mother and scrutinized her baby. He seemed to be the epitome of good health. He did not look famished or ‘deficient’ in any way. He was healthy to a fault. According to his mother, he hardly fell ill, not even with a common cold.
This mother encouraged new moms to breastfeed exclusively for six months. She was a career mother and had managed to do so. Interesting, I thought, especially because I knew I would be a working mother myself.
Included in the news segment were a peditrician and a nutritionist, both of whom affirmed that breastmilk only was best for baby for the first six months. They said breastmilk contained all the nutritional components needed for a baby’s growth for the first six months.
These people had to be kidding. Even professionals were in agreement with this woman?
I decided that additional research was necessary. I Googled and Googled and Googled some more. It was unanimous: breast milk is best. I began thinking that I would give it a try.
By the time my son arrived two months later in April 2011, I was sold. I exclusively breast fed him for six months, even after I returned to full-time work when he was three months old. I carried a breast pump to work, and expressed milk over my lunch hour. It was the first time my decade-old company had received a request for space to pump. The storeroom, filled with old newspapers, was the best they could offer me.
Suffice it to say that I also managed to exclusively breastfeed my second son, born in April, 2013.
The benefits of exclusive breastfeeding have been well worth it. My sons don’t fall ill often. We saved a significant amount of money because we didn’t have to buy formula, which I would have done if I had not succeeded in exclusively breastfeeding them both. Today, I use all channels within my disposal to campaign for exlusive breastfeeding because I believe it is the best start a mother can give her child.
Just the other day, I was happy to learn that the exclusive breastfeeding rates in Kenya have gone up from 32% six years ago to 61%. Meaning that I and all the other mothers I have managed to inspire through my blog and other advocacy campaigns are among the counted! Yaaaay! That has been the greatest news I have heard in a long while.
Higher rates of exclusive breastfeeding mean that more children get to survive their infancy, fall ill less often, and get to celebrate their first birthdays.
I believe that giving a child a healthy start to life through a good nutritional foundation is one of the best gifts you can offer your child. My sons appear to agree!
Is exclusive breastfeeding common where you live?
This is a post original to World Moms Blog by Maryanne W. Waweru of Mummy Tales in Kenya. Photo credit to the author.
Maryanne W. Waweru, a mother of two boys, writes for a living. She lives in Nairobi, Kenya with her family. Maryanne, a Christian who is passionate about telling stories, hopes blogging will be a good way for her to engage in her foremost passion as she spreads the message of hope and faith through her own experiences and those of other women, children, mums and dads. She can be found at Mummy Tales.
More Posts - Website

by World Moms Blog | May 7, 2015 | 2015, Awareness, Being Thankful, Birthing, Casting a Wider Net, Clean Birth Kits, Education, Global Citizenship, Health, Helping, Human Rights, International, Life, Life Lesson, Loss of Child, Maternal Health, Motherhood, Newborn Health, ONE, Pregnancy, Priorities, Responsibility, Tragedy, Transportation, Womanhood, Women's Rights, Working Mother, World Mom Feature, World Motherhood
 Every mother has the right to access the care they need during pregnancy and childbirth – care that can identify, prevent, and manage complications should they arise. But failure to meet these needs results in the loss of 800 mothers every day, even though up to 98% of these deaths are preventable.
Every mother has the right to access the care they need during pregnancy and childbirth – care that can identify, prevent, and manage complications should they arise. But failure to meet these needs results in the loss of 800 mothers every day, even though up to 98% of these deaths are preventable.
Every Mother Counts is working to provide solutions that can make pregnancy and childbirth safer. We know that with the right care at the right time, it IS possible that every mother could have the chance to survive and thrive.
Recently, World Moms Blog sat down with Executive Director of Every Mother Counts, Erin Thornton, to talk about how she got involved with the organization and what drives her to work so hard for maternal health.
World Moms Blog: Erin, you’re the mother of three young girls and you live in the metro-Boston area yet you are the executive director of Every Mother Counts, a New York-based non-profit working in five locations around the world. How did you get involved?
Erin Thornton: My involvement with Every Mother Counts grew out of a 10-day trip to Africa with my former organization, ONE. We had invited Christy Turlington Burns along and she and I got chatting about maternal health. Maternal health was not an issue ONE focused on and I was really drawn to what Christy was telling me about.
WMB: What about maternal health drew you in?
ET: Well, Christy had just completed the film, “No Woman, No Cry” a documentary about maternal health challenges that impact the lives of millions of girls and women around the world. During our trip through five African countries, Christy and I spent a lot of time comparing notes on what was needed to move the maternal health agenda forward. Through all my time at ONE, I realized how interlinked so many poverty challenges are to maternal health—that if moms are kept alive, we can better keep kids alive, better give them an education and clean water, etc. Yet still no one was really talking about it.
WMB: What prompted you to leave behind a long career with ONE and join Christy in her pursuit of spreading maternal health awareness as she built this new non-profit?
ET: I had been with ONE since 2002, when I became the first hire in the US for ONE’s predecessor organization, DATA. By 2010, ONE had grown to 120 people in four different global offices. I had two young girls and I was starting to think about making a change. The more Christy and I talked about the need for an “awareness campaign” for maternal health, the more I realized I wanted to be a part of it too, so six-months later, I formally signed on to help her build the organization.
WMB: In just a few days (May 10), we celebrate Mother’s Day here in the US, can you share with World Moms something about what makes you a passionate believer in Every Mother Counts?
ET: Physiologically, every woman goes through pregnancy the same way and faces the same chances of developing a complication. The difference in how they fare mainly comes down to whether they have access to good health care- or not. Helping more moms enjoy a safe pregnancy and delivery may sound like an overwhelming challenge but we really CAN make a difference. EMC has identified three target areas to focus our support on: 1. transport, 2. education and training for healthcare providers, and 3. supplies for clinics–including birth kits, solar suitcases and lighting. And we’re seeing that these seemingly simple things are making a big difference.
This Mother’s Day, Every Mother Counts is celebrating #WhatIsPossible for every mother.
Every mother has the right to access the care they need during pregnancy and childbirth – care that can identify, prevent, and manage complications should they arise. But failure to meet these needs results in the loss of 800 mothers every day, even though up to 98% of these deaths are preventable.
Every Mother Counts is working to provide solutions that can make pregnancy and childbirth safer. We know that with the right care at the right time, it IS possible that every mother could have the chance to survive and thrive.
So this Mother’s Day, as we look at the future of maternal health, we ask ourselves #WhatIsPossible? And the answer is, a lot.
With your help, Every Mother Counts has already impacted thousands of lives by improving access to critical maternal health care for vulnerable mothers.
During the month of May, we invite you to spread the good news about by sharing this .
This is an original interview with Erin Thornton posted by World Moms Blog Managing Editor, Kyla P’an.
The image used in this post is from the Every Mother Counts website and is used here with permission.
World Moms Blog is an award winning website which writes from over 30 countries on the topics of motherhood, culture, human rights and social good. Over 70 international contributors share their stories from around the globe, bonded by the common thread of motherhood and wanting a better world for their children.
World Moms Blog was listed by Forbes Woman as one of the "Best 100 Websites for Women 2012 & 2013" and also called a "must read" by the NY Times Motherlode in 2013. Our Senior Editor in India, Purnima Ramakrishnan, was awarded the BlogHer International Activist Award in 2013.
More Posts

by Kristyn Zalota | Apr 21, 2015 | 2015, Awareness, Babies, Birthing, Clean Birth Kits, Humanitarian, Inspirational, Laos, Motherhood, Newborn Health, Philanthropy, Social Good, World Moms Blog, World Voice
The Truth About Fundraising.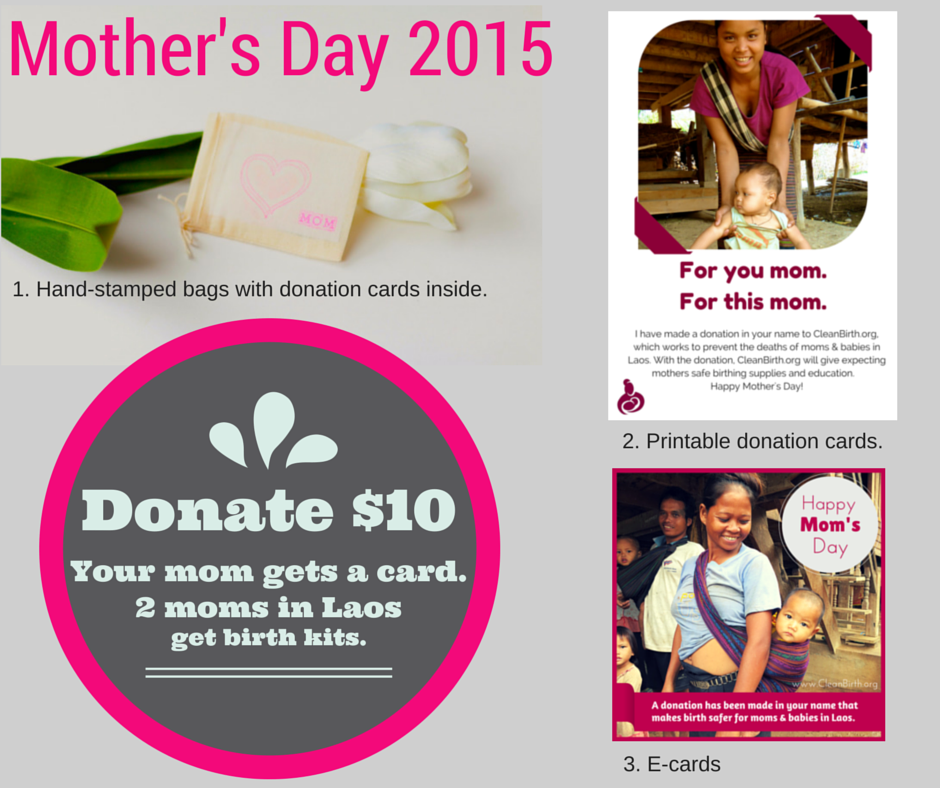
When I talk about the fundraising work that I do for the organization I started, CleanBirth.org, I often hear in response, “I could never ask people for money.”
I’ll be honest, I don’t have a choice. When I began providing moms with life-saving birth supplies, in partnership with a local NGO in Laos, I used my own funds. Happily, the $5 kits proved effective and more moms wanted the sterile, convenient supplies that prevent deadly infections in moms and babies. How could I say no?

So I promised to fund as many kits as were needed.
Since we began in November 2012 we have provided 4,000 birth kits to moms and training for 180 nurses and staff.
Knowing that my own funds couldn’t sustain the project, I told my story to others. I wasn’t great at promoting the project at first but many friends and family supported me anyways. The tagline: $5 Saves 2 Lives in Laos proved irresistible.
Now 3 years on, the project has grown beyond my own social network. Thanks to bloggers at World Moms Blogs and others, we have extended our reach worldwide. I am constantly touched by the simple notes of support that accompany donations from complete strangers:
Thank you for doing what you do for mothers and babies!

Another great aspect of fundraising is working with others who want to share their special gifts to make birth safer. One example is a fun collaboration happening now for Mother’s Day. World Moms Blogger and photographer Ewa Kuc of Ewa Samples Photography in the Bay Area has developed awesome Mother’s Day photo session packages. A full 40% of the profits go to CleanBirth.org!
In my almost 3 years doing this, I have come to appreciate that fundraising is a give and take proposition.
I’m not just taking money but giving something to donors: a feeling of making a positive impact in the world; the piece of mind that comes from donating to a transparent, registered organization; or a tangible gift to give a loved one.
One such gift, our $10 Mother’s Day cards, honor mom or grandma & provide 2 moms in Laos with Clean Birth Kits.
So the truth about fundraising is that I do ask for money. (Please click here to buy our Mother’s Day cards!! J) But I also get to connect with many generous people who are committed to making their world a better place. We each give, and we each take. Not so scary after all.

What benefits do you receive from donating or volunteering with a non-profit?
This is an original post written for World Moms Blog by Kristyn Zalota, the founder of Clean birth.org
Photo credits Kristyn Zalota.
Kristyn brings her years of experience as an entrepreneur and serial volunteer to CleanBirth.org. She holds a MA, has run small businesses in Russia and the US, and has volunteered in Nicaragua, Costa Rica, Thailand, Cambodia, Laos and Uganda on projects related to women’s empowerment.
After having children, Kristyn became an advocate for mothers in the US, as a doula and Lamaze educator, and abroad, as the Founder of CleanBirth.org. She is honored to provide nurses in Laos with the supplies, funding and training they need to lower maternal and infant mortality rates in their villages.
More Posts

by Elizabeth Atalay | Jun 24, 2014 | 2014, Africa, Awareness, Babies, Birthing, Ethiopia, Health, Humanitarian, Maternal Health, Millennium Development Goals, Motherhood, Newborn Health, Pregnancy, Save The Children, Social Good, Third Eye Mom, Travel, World Moms Blog, World Voice

We had just spent the night at the source of the Blue Nile River. Lake Tana sits in Bahir Dar, Ethiopia, and as our caravan of Land Cruisers wove through the countryside from Bahir Dar to Mosebo I took in deep gulping breaths of sweet fresh Ethiopian air. The lush colors of our surroundings looked to me like they had been enhanced in Photoshop in the way that everything seemed to pop. How could I feel this emotional connection to place that was never mine? A place I had never been?
Though this is my first time in Ethiopia, the verdant landscape brought me back to other rural parts of Africa I’d traveled through in my youth, similar topographies that had stayed with me ever since. This time I’d returned to the continent as a new media fellow with the International Reporting Project to report on newborn health. World Moms Blog Editor Nicole Melancon of ThirdEyeMom is a fellow on the trip as well, and last week wrote about our initial overview of maternal and newborn health in Ethiopia. Now we were heading to one of the villages housing a Health Post, which serves the local and surrounding population of approximately 3,500 people.

Mosebo Village is part of Save The Children’s Saving Newborn Lives program, and as such is looked to as a model village in the Ethiopian Government’s plan to reduce maternal and newborn mortality. Mosebo is a rural agrarian community that produces wheat, teff and corn. There I met seven-year-old Zina whose mother, Mebrate was about to give birth. Through our translator Mebrate estimated her age to be around 26, and told us that Zina was her first child. For economic reasons she and her husband had waited to have a second. When she had Zina, Mebrate had gone to her parent’s home to give birth, as women in Ethiopia often do. It is estimated that 80% of Ethiopian mothers will give birth in their home, often without a trained health care attendant. Towards the end of Mebrate’s first pregnancy she went to live with her parents as her family instructed, until after the baby was born. In that way her mother could help her deliver, could care for her and the baby, and feed her the traditional porridge after birth. Although there were no complications during her delivery, sadly, many young mothers giving birth at home are not as fortunate. The time period during and around birth are the most vulnerable for the lives of both the mothers and babies. The Saving Newborn Lives Program aims to reduce maternal and newborn mortality beginning with awareness programs and antenatal care on the local level at Health Posts like the one we visited in Mosebo.

The Mosebo Health Post and Health Extension Workers
We had met Tirgno and Fasika, the two Health Extension Workers at the Mosebo Health Post earlier that day as they showed us the two room interior, and explained their role in improving maternal and newborn health. They work to raise awareness in the community about the importance of antenatal care, and the potential dangers of giving birth at home for both mother and child. Newborn health is interdependent with maternal health, and the most prevalent causes of newborn mortality, infection, Asphyxiation, pre-maturity or low birth weight, and diarrhea can often be avoided with proper care. These days in Mosebo after receiving antenatal care at the Health Post women are then referred to the regional Health Center for deliveries.

Zina shyly smiled when we ask her how she felt about having a new sibling, she stood straight and tall listening intently as we asked her mother about the babies’ arrival. When Mebrate goes into labor this time, with her second child, she will embark on the walk along rural dirt roads for around an hour to the nearest Health Center to give birth.
Elizabeth Atalay is reporting from Ethiopia as a fellow with the International Reporting Project (IRP). This is an original post written for World Moms Blog.
You can follow all IRP reports by World Moms Elizabeth Atalay & Nicole Melancon at #EthiopiaNewborns

Elizabeth Atalay is a Digital Media Producer, Managing Editor at World Moms Network, and a Social Media Manager. She was a 2015 United Nations Foundation Social Good Fellow, and traveled to Ethiopia as an International Reporting Project New Media Fellow to report on newborn health in 2014. On her personal blog, Documama.org, she uses digital media as a new medium for her background as a documentarian. After having worked on Feature Films and Television series for FOX, NBC, MGM, Columbia Pictures, Warner Brothers, 20th Century Fox, and Castle Rock Pictures, she studied documentary filmmaking and anthropology earning a Masters degree in Media Studies from The New School in New York. Since becoming a Digital Media Producer she has worked on social media campaigns for non-profits such as Save The Children, WaterAid, ONE.org, UNICEF, United Nations Foundation, Edesia, World Pulse, American Heart Association, and The Gates Foundation. Her writing has also been featured on ONE.org, Johnson & Johnson’s BabyCenter.com, EnoughProject.org, GaviAlliance.org, and Worldmomsnetwork.com. Elizabeth has traveled to 70 countries around the world, most recently to Haiti with Artisan Business Network to visit artisans in partnership with Macy’s Heart of Haiti line, which provides sustainable income to Haitian artisans. Elizabeth lives in New England with her husband and four children.
More Posts

by Nicole Melancon (USA) | Jun 17, 2014 | 2014, Ethiopia, Humanitarian, Maternal Health, Newborn Health, Save The Children, World Voice

Ethiopia, one of the poorest countries in Africa with a population of 90 million people, stunned the world by achieving the Millennium Development Goal #4 of reducing the mortality rates of children under age 5 by two-thirds well ahead of the 2015 deadline. In a country in which 95% of the population lives outside of an urban center in rural, remote and hard to reach areas and a shocking 80% of women birth at home without a midwife. Health Extension Workers (HEW) have been the key ingredient to Ethiopia’s success. However, sadly the rate of newborn survival in Ethiopia has not shown nearly as much progress.
As an international reporting fellow with The International Reporting Project, fellow World Moms Blog editor, Elizabeth Atalay, and I are in Ethiopia for the next two weeks reporting on newborn health. We will be meeting with a diverse variety of people around the country such as doctors, health officials, mothers, NGOs, midwives and health extension workers to learn about Ethiopia’s maternal, newborn and child health systems, policies and strategies for improving newborn health. Today we had a presentation on maternal, newborn and child health in Ethiopia given by Dr. Abeba Bekele, the Program Manager at Save the Children Ethiopia’s Saving Newborn Lives Program.
Dr. Abeba Bekele is a medical doctor by training yet after spending five years working in the field she saw firsthand some of the tragic problems with maternal care in her country.
Watching as a patient bled to death after delivery, and being unable to save this mother of six, was a turning point for Dr. Abeba. She decided to move to working in public health policy in hope of improving Ethiopia’s poor maternal and child health care system.
Over the years, Dr. Abeba has seen remarkable progress in some areas, but painfully slow progress in other areas in regards to maternal, newborn and child health.
- Over the past 20 years, Ethiopia has reduced child deaths (for children under age 5) by more than two-thirds. In 1990, an estimated 204 children in every 1,000 in Ethiopia died before the age of five. Now that number is closer to 69 in every 1,000.
- While 1- 59 months (i.e. 5 year) child mortality rate is declining 6.1% annually the neonatal rate (first 28 days of life) is only declining 2.4% annually.
- Since the year 2000, Ethiopia has reduced its lifetime risk of maternal death from 1 in 24 to 1 in 67.
Although these figures are encouraging, there is also much work to be done in improving maternal, newborn and child health in Ethiopia. One of the main issues that is making maternal and newborn mortality rates difficult to tackle is the fact that over 80% of women in Ethiopia deliver at home with no trained help. These women give birth assisted by the community birth attendant, with a friend, a neighbor or even by themselves. The best way to save both maternal and newborn lives is to have women give birth assisted by a trained midwife at a health center. In fact the Ethiopian government is strongly encouraging all women to give birth at a health center but there are many obstacles in the way.

In an effort to improve maternal, newborn and child health, the Ethiopian government has implemented a massive effort of new policies and programs throughout the nation. The biggest success story has been the training and deploying of an army of 34,000 Health Extension Workers (HEW). Implemented in 2005, this massive effort has had remarkable success in saving lives through education, prevention of diseases, and provision of family health services. HEW’s live within the community and are trained and paid by the government to do home visits for an assigned population within their community. HEWs have been successful in cutting child under five deaths significantly as they can check and treat for the biggest child killers like diarrhea, pneumonia and malaria. However, HEWs are not trained as midwives, and can only advise a woman to give birth in a health center. This is an area that must be changed as giving birth by a trained professional in a health center would significantly reduce neonatal and maternal deaths.
Progress also needs to be made in the sheer accessibility and number of health centers. Today there are only 3,500 health centers in Ethiopia for 90 million people. More health centers and hospitals need to be built and more roads to reach the inaccessible areas. More midwives need to be trained and distributed throughout the country. According to the 2012 State of the World’s Midwives report, there is one midwife for every 18,000 people in Ethiopia whereas the World Health Organization recommends there should be one midwife per every 5,000 people in a given country. A lot of work needs to be done but the progress they have made in the past two decades is admirable.
Nicole Melancon is reporting from Ethiopia as a fellow with the International Reporting Project (IRP). This is an original post written for World Moms Blog.
You can follow all IRP reports by World Moms Elizabeth Atalay & Nicole Melancon at #EthiopiaNewborns

Third Eye Mom is a stay-at-home mom living in Minneapolis, Minnesota with her two children Max (6) and Sophia (4). Her children keep her continually busy and she is constantly amazed by the imagination, energy and joy of life that they possess! A world wanderer at heart, she has also been fortunate to have visited over 30 countries by either traveling, working, studying or volunteering and she continues to keep on the traveling path.
A graduate of French and International Relations from the University of Wisconsin Madison, where she met her husband Paul, she has always been a Midwest gal living in Minnesota, Wisconsin and Chicago. This adventurous mom loves to be outside doing anything athletic (hiking, running, biking, skiing, snowshoeing or simply enjoying nature), to travel and volunteer abroad, to write, and to spend time with her beloved family and friends.
Her latest venture involves her dream to raise enough money on her own to build and open a brand-new school in rural Nepal, and to teach her children to live compassionately, open-minded lives that understand different cultures and the importance of giving back to those in need. Third Eye Mom believes strongly in the value of making a difference in the world, no matter how small it may be. If there is a will, there is a way, and that anything is possible (as long as you set your heart and mind to it!).
Visit her on her blog, Thirdeyemom, where she writes about her travels and experiences in other lands!
More Posts

by Dee Harlow (Laos) | May 29, 2014 | Awareness, Breastfeeding, Food, Health, Humanitarian, Laos, Maternal Health, Millennium Development Goals, Nutrition, Uncategorized, World Voice, Younger Children
 While I still have the opportunity to write another post for the WMB community before leaving Laos later this year, I feel compelled to tell you about child nutrition and the problem of stunting in Laos because stunting is a seemingly invisible problem that can go unnoticed unless special attention is drawn to highlight the issue.
While I still have the opportunity to write another post for the WMB community before leaving Laos later this year, I feel compelled to tell you about child nutrition and the problem of stunting in Laos because stunting is a seemingly invisible problem that can go unnoticed unless special attention is drawn to highlight the issue.
Ethnically, most Southeast Asian people are shorter and have a smaller frames than most other races throughout the world. This fact makes it easy to say that Lao babies and children tend to be small or smaller because of their race.
Yet at first glance Lao children appear to be healthy (and super cute), a closer look and personal interaction will almost always reveal that the children are a few years older than what you had first assumed. I recently met an adorable girl in a northern village at a school where I delivered books by boat since there is no road access to her village. Upon speaking with her (in Lao) I was impressed by how well behaved, articulate and “mature” she was for what I assumed to be a 6-year old. (I have two 4-year old twins so I was instantly optimistic about their potential in just two short years to be as well behaved as this girl.) She turned out to be 10-years old. This has happened time and time again to me, to my colleagues, and to many newcomers to Laos.
Lao children are among the most undernourished in Southeast Asia with 44% stunting of children under 5-years old. It is the single largest contributor to infant and child mortality in the country with 59% of all child deaths related to nutritional deficiencies. Chronic malnutrition predisposes children to higher morbidity and mortality, lower educational attainment, and reduced workforce productivity.
For a country experiencing rapid economic growth and increasing income disparities, fierce external human resource competition puts the country at risk of leaving a majority of the Lao population behind others who will be more able to keep apace. Stunting is a problem that needs be addressed for the immediate wellbeing of Lao children and to be resolved for the future potential of the Lao people.
The Lao government is working closely with experts and development partners on how to tackle this important issue. It is not easy. Poor breast-feeding and weaning practices are widespread. Almost all mothers give food supplements (such as chewed glutinous rice), and pure water, to infants within a few weeks of birth. Harmful practices (such as discarding colostrum) and other food taboos for pregnant women reduce disease resistance for newborns and increase fetal undernutrition. Micronutrient deficiencies, inadequate intake of vitamin A, anemia and iodine deficiency, all further hinder child development.
The current health system is not only faced with challenges of delivering micronutrients, immunizations and necessary vitamins to the most vulnerable population, but they are additionally burdened by the daunting task of changing people’s behaviors to improve dietary habits, increase nutritional intake, and overcoming cultural belief and religious belief obstacles to improved nutrition status among rural and multi-ethnic communities. The task is daunting.
What is being done and what needs to be done?
There are some great organization here making slow but successful strides on a small-scale basis. UNICEF, WFP, IFAD, Save the Children, the Scale Up Nutrition initiative and others who are collaborating closely with government health officials, but resources are scarce, especially in an often overlooked country like Laos.
- We can channel financial support to these organizations for their work on nutrition in Laos.
- We can lobby our governments to increase foreign assistance resources to address the poor state of healthcare in Laos (e.g., Laos is not one of the United States’ ‘priority countries’ receiving Global Health Initiative (GHI) funding. Ask U.S. representatives, Why not?)
- We can voice our concern to private and public interests who are taking advantage of opportunities in Laos to improve their social welfare practices by investing in better healthcare in communities where they pursue their business interests.
- We can ask the question to anyone willing to listen about who should be accountable to improving the welfare of children beginning their lives under such great odds in Laos.
Hopefully someday, someone will listen and take action.
This is an original post to World Moms Blog by our mother of twins writer, Dee Harlow in Vientiane, Laos. You can always find her writing on her blog, Wanderlustress.
Photo credit attributed to the author.
One of Dee’s earliest memories was flying on a trans-Pacific flight from her birthplace in Bangkok, Thailand, to the United States when she was six years old. Ever since then, it has always felt natural for her to criss-cross the globe. So after growing up in the northeast of the US, her life, her work and her curiosity have taken her to over 32 countries. And it was in the 30th country while serving in the Peace Corps in Uzbekistan that she met her husband. Together they embarked on a career in international humanitarian aid working in refugee camps in Darfur, Sudan, and the tsunami torn coast of Aceh, Indonesia.
Dee is now a full-time mother of three-year old twins and continues to criss-cross the globe every two years with her husband who is in the US Foreign Service. They currently live in Vientiane, Laos, and are loving it! You can read about their adventures at Wanderlustress.
More Posts

 Exclusive breastfeeding. Before I became a mother, I had never heard of it. I knew about breastfeeding, obviously, but not until I was seven months pregnant with my first child, did I learn it was possible to feed a baby only breastmilk for six months.
Exclusive breastfeeding. Before I became a mother, I had never heard of it. I knew about breastfeeding, obviously, but not until I was seven months pregnant with my first child, did I learn it was possible to feed a baby only breastmilk for six months.